Long-Term Efficacy of a Methacrylate Resin-Based Root Canal Sealer
Ten-year retrospective study results with EndoREZ.
Long-term success of root canal treatment depends on many factors in which a sealer plays an important role. Numerous studies have been published reporting endodontic outcomes using clinical and radiographic methods.1-5 The retrospective study reported below was conducted on an initial patient pool of 180 patients6 with 295 root canals filled with laterally condensed gutta-percha and EndoREZ® (Ultradent Products, Inc., www.ultradent.com), a methacrylate resin-based endodontic sealer.
After 14 to 24 months, 145 patients were evaluated. An overall success rate of 91% was reported.6 In a follow-up study 5 years later, 120 patients were evaluated, and a success rate of 90% was reported. This brief offers a condensed version of a report on 10-year postoperative data of the same patient pool.7
Materials and Methods
Of the original 180 patients (age range 12 to 75 years) treated during a single visit in a private practice setting, 89 patients with 175 root canals responded to a 10-year recall examination and were clinically and radiographically evaluated.
Clinical Protocol
Preoperative radiographs were taken during the initial treatment, and the health of pulp and periradicular areas were recorded. Under local anesthesia and rubber dam isolation, the pulp chamber was accessed. After hand instrumentation with a crown-down technique for radicular access, a step-back technique was used for apical preparation. The coronal two thirds were flared with #1 through #3 Gates Glidden drills (DENTSPLY Maillefer, www.maillefer.com). Then the working length was established with a #15 file, approximately 1 mm short of the radiographic apex. Canal preparation was done with K-type and Hedström files (DENTSPLY Maillefer) at the apical third to a master apical #30 to #40 file and coronally to a #60 file. Patency was confirmed with a #10 K-file. Irrigation was performed after every change of instrument with 2.5% sodium hypochlorite, followed by ethylenediaminetetraacetic (EDTA) acid. A final rinse with saline completed the treatment. With sterile paper points, the canals were lightly dried to take maximum advantage of the hydrophilic properties of the resin sealer. (The last paper point showed at least 3 mm of moisture.) EndoREZ (ER) and lateral compacted gutta-percha sealed the canals. Access cavities were sealed with IRM® (DENTSPLY Caulk, www.caulk.com), and the patients returned to their restorative dentist for definitive care.
The follow-up evaluation consisted of a clinical examination (percussion) and radiographs, the latter by two experienced calibrated endodontists. The level of the root canal fillings in relation to the working length was recorded, and the quality of the root fills were judged adequate when they were placed to the full working length without voids. Canals that did not meet these conditions were categorized as “filled short” or “inadequate.” Failure of one canal in multi-rooted teeth was a considered to be complete failure. In cases with apical radiolucencies, the size of the lesions were measured on the radiographs as being < 2 mm or > 2 mm. Success or failure of the endodontic treatment was determined on the basis of radiographic findings and clinical signs and symptoms according to the criteria explained below.
Outcome of Treatment
Success
The treatment was considered to be successful if radiographically, the contours and width of the periodontal ligament (PDL) space were within normal limits or slightly widened around an accidental overfill, and the patient was free of symptoms. Slight tenderness to percussion for a brief postoperative period was considered acceptable.
The size of a preoperative radiolucent area decreased by at least 50% and the patient was free of symptoms, or the contours and width of the PDL space had returned to normal. Lastly, if there was an absence of preoperative periapical radiolucency, which remained unchanged over time, the case would be declared a success.
Failure
Treatment failure was considered when a periapical radiolucency was observed in the preoperative radiograph and remained unchanged or increased in size over time; or a root that, in the absence of preoperative periapical pathosis, developed a radiolucency over time.
Results
The correlation of treatment outcomes with respect to age, gender, and specific preoperative and postoperative data were analyzed by the Fisher exact test (P < .05). For the censored data—ie, the total number of patients who did not respond to the previous 14- to 24-month and 5-year recalls (35 and 25, respectively)—a life table survival analysis was performed to determine the cumulative probability of success. A corresponding 95% confidence interval (CI) was determined.
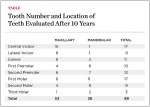
Analysis of the inter-examiner calibration demonstrated a ratio of 93%, indicating a strong inter-observer agreement. A total of 89 patients (49.44%) with 178 treated root canals presented for the 10-year evaluation. The number and location of teeth are shown in the Table.
Seventy-eight teeth (87.64%) were evaluated as adequately filled to working length. In five cases (5.61%), the apical limit of the root-filling material was found to be short of working length. Four (4.49%) of these, which were filled flush at the time of endodontic treatment, underwent resorption of the sealer within the lumen of the canals showing root fills ± 1 mm from the radiographic apex. Two cases (2.24%) with immediate postoperative extrusion showed no evidence of sealer in the periradicular tissues. Forty-two teeth (47.19%) with preoperative vital pulps were successful in 38 cases, while 47 (52.80%) with preoperative non-vital pulps, were successful in 44 cases. Of these cases, five in which a slight widening of the PDL space was noted, were initially classified as doubtful; however, these patients were asymptomatic. The remaining three cases showed a wide periapical radiolucent area, which was not present at the time of the treatment. Thirty-nine teeth (43.82%) showing preoperative periapical radiolucencies revealed almost total or total healing in 36 cases, while three presented with some discomfort and showed persistent radiolucencies (rated as failures). In total, seven teeth were considered clinically and radiographically to be failures. The differences in the outcome of treatments related to age, gender, preoperative pulp or periapical status, the size of periapical lesions, and the type of permanent restorations were not statistically significant (P > .05). The life table analysis revealed a cumulative probability of success of 92.13% at the 10-year recall, with a 95% CI of 83 to 94.
Clinical Significance
Using a method of evaluating patients following a predetermined clinical and radiographic protocol is considered a reliable procedure when evaluating the outcome of endodontic treatment,2-4 especially because the same evaluation criteria are being used by clinicians. This was further enforced by two recent histological investigations8,9 that demonstrated a good correlation between radiographic success and the histological features of the periapical tissues in humans.
Twenty-three (25.84%) patients did not respond to the recall. Reasons for declining the recall included lack of interest or time, pregnancy, general diseases, death, or relocation. Of these 23 patients, three had the tooth in question extracted because of a root fracture. All three teeth had a cast post-and-core and were restored with a crown.
Of significance is that extrusion of ER, which accidentally occurred in 10 cases at the initiation of the study, did not adversely affect the outcome of treatments. After 10 years, these cases appeared radiographically normal without evidence of sealer in the periapical tissues. Whether treated in single or multiple visits, the outcome of treatment was not significantly different.
Conclusion
The results of this study suggest that ER used in conjunction with gutta-percha constitutes an acceptable root canal filling procedure and is comparable to findings published by other authors evaluating different sealers.
Disclosure
Dr. Pameijer is a consultant for Ultradent.
References
1. Grossman LI, Shepard LI, Pearson LA. Roentgenologic and clinical evaluation of endodontically treated teeth. Oral Surg Oral Med Oral Pathol. 1964;17:368-374.
2. Heling B, Tamshe A. Evaluation of the success of endodontically treated teeth. Oral Surg Oral Med Oral Pathol. 1970;30(4):533-536.
3. Barbakow FH, Cleaton-Jones P, Friedman D. An evaluation of 566 cases of root canal therapy in general dental practice. 2. Postoperative observations. J Endod. 1980;6(3):485-489.
4. Swartz DB, Skidmore AE, Griffin JA Jr. Twenty years of endodontic success and failure. J Endod. 1983;9(5):198-202.
5. Friedman S, Löst C, Zarrabian M, Trope M. Evaluation of success and failure after endodontic therapy using a glass ionomer cement sealer. J Endod. 1995;21(7):384-390.
6. Zmener O, Pameijer CH. Clinical and radiographic evaluation of a resin-based root canal sealer. Am J Dent. 2004;17(1):19-22.
7. Zmener O, Pameijer CH. Clinical and radiographic evaluation of a resin-based root canal sealer: 10-year recall data. Int J Dent. 2012; Article ID 763248, doi:10.1155/2012/763248
8. Green TL, Walton RE, Taylor JK, Merrell P. Radiographic and histologic periapical findings of root canal treated teeth in cadavers. Oral Surg Oral Med Oral Pathol Oral Radiol Endod. 1997;83(6):707-711.
9. Ricucci D, Lin LM, Spångberg LS. Wound healing of apical tissues after root canal therapy: a long-term clinical, radiographic and histopathologic observation study. Oral Surg Oral Med Oral Pathol Oral Radiol Endod. 2009;108(4):609-621.
Commentary by Howard E. Strassler, DMD
Professor, Division of Operative Dentistry
Department of Endodontics
Prosthodontics and Operative Dentistry
University of Maryland Dental School
Baltimore, Maryland
Commentary
In the past decade we have seen changing trends in the types of sealers used in endodontic treatment. While excellent biomechanical preparation is required as part of endodontic treatment, clinical success also relies on numerous elements being completed correctly. To achieve a positive outcome with endodontic treatment, the type of sealer used and its correct use is very important. This well-done clinical study evaluated a new class of endodontic sealer that is methacrylate resin-based. The inclusion criteria for this study included vital and non-vital teeth including teeth with preoperative periapical radiolucencies. Most clinical studies end at 3 to 5 years. This clinical study evaluated the results using the EndoREZ methacrylate resin-based root canal sealer over 10 years. For the patients recalled, 89 patients with 175 root canals, the researchers reported a 92% success rate at 10 years. From this study, a clinician can select the use of EndoEz root canal sealer with a high level of confidence.
About the Authors
Osvaldo Zmener, DDS, Dr.Odont
Head Professor, Post Graduate Program for Specialists in Endodontics
School of Dentistry, University of El Salvador
Buenos Aires, Argentina
Cornelis H. Pameijer, DMD, MScD, DSc, PhD
Professor Emeritus
University of Connecticut School of Dental Medicine
Farmington, Connecticut
Private Practice
Farmington, Connecticut