Endodontics in General Practice
Meeting the new standard of care
Sefira Fialkoff
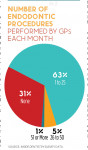
More than two-thirds of general practitioners (GPs) who responded to an Inside Dentistry survey reported that they perform endodontic procedures. They indicated that, primarily, they perform standard root canal treatments, with smaller percentages indicating that they handle retreatments (15%), root canal obstructions (6%), and apexification procedures (5%). Oftentimes, endodontists support the idea of GPs doing some of this work—provided that they possess sufficient education and experience and that the cases that they handle aren't too complex. But where is the line between what can be kept in-house by a general practice and what should be referred to a specialist? How is that line defined, and what factors continue to move it?
Drawing the Line
Unfortunately, there is no established system for deciding exactly which cases are best referred to an endodontist and which can be managed by a GP. The simpler the case, the easier it may be for a GP to perform the treatment. "The problem is that there are no hard-and-fast rules for determining what is going to be a simple endo case," explains Rebekah Lucier Pryles, DMD, an assistant clinical professor of endodontics at the Tufts University School of Dental Medicine and private practitioner in White River junction, Vermont. "For example, a lot of us believe that anterior teeth are the most straightforward to treat, but in my clinical experience, they can be some of the most difficult. Therefore, the only hard-and-fast rule is that GPs must know their own limitations."
The American Association of Endodontists (AAE) provides an Endodontic Case Difficulty Assessment Form and Guidelines that can be used by clinicians to consider factors that may impact the difficulty of treatment. Using the form, cases are categorized as low, moderate, or high difficulty based upon risk factors that may complicate treatment. The more potentially complicating factors that are involved (eg, malalignment, reduced canal size, canal obstructions, calcifications, curvature, etc), the more difficult the case, which increases the recommendation to refer. "Generally, a great place to start into endodontics is with anterior single-canal cases," suggests Melissa Seibert, DMD, MS, a US Air Force dentist and deputy AEGD program director at Langley Air Force Base in Hampton, Virginia, and a clinical instructor at Creighton University School of Dentistry in Omaha, Nebraska. "With more experience, practitioners can move on to premolars, followed by molars and retreatments."
The expectation to meet the standard of care is the same for GPs as it is for endodontists. That level of accountability, as well as the speed and efficiency with which the service can be provided and other factors, should play into the calculus that every provider does for each case. "It's not just about looking at a tooth on a radiograph," says Pryles. "We must consider the whole patient."
"What's important to note is that the tooth itself matters, of course, but so do factors related to how the patient can tolerate treatment," agrees Brooke Blicher, DMD, an assistant clinical professor of endodontics at the Tufts University School of Dental Medicine and private practitioner in White River junction, Vermont. "For example, molars have more complex anatomy that is worthy of the specialized training and equipment of a specialist, but anterior teeth that have full-coverage restorations or demonstrate evidence of calcification may require the same. Similarly, patients who are unable to sit for long procedures or those with limited openings or strong gag reflexes may have better experiences with specialist care due to efficiencies, expertise, and in some cases, the specialist's ability to perform the treatment with the aid of an anesthesiologist for sedation."
Like many specialists, Blicher receives a range of referrals. Some referrers send everything her way, whereas others only send molars and more complex cases. Some send almost nothing her way unless their attempts are unsuccessful. "Of course, these latter cases are the trickiest," explains Blicher. "Oftentimes, my consultation turns into an awkward dance of me pointing out complications that were unrecognized in the unsuccessful attempt to deliver care, such as a perforation, a separated instrument, or an otherwise overextended access that risks fracture. Obviously, I'd prefer that these cases be sent to me from the beginning-not only to reduce the awkward encounters but also to improve our chances of saving teeth!"
Ideally, GPs should be able to critically evaluate their own competency as diagnosticians and clinicians and identify areas for which they require additional educational experiences. In doing so, they should not undertake a case unless they are prepared to also manage any complications that may arise during treatment. "Mandibular premolar teeth are infrequently multi-rooted, but that can be hard to see without utilizing certain technology," explains Pryles.
Regarding complications, endodontic re-treatments can also present complexity. "There are many reasons why a tooth may require re-treatment, such as a missed canal, over- or under-obturation, a perforation, etc," Seibert adds. "But if you can't determine whether or not the tooth needs re-treatment or how best to handle it, you should refer it."
Chad Duplantis, DDS, a fellow of the Academy of General Dentistry and private practitioner in Fort Worth, Texas, explains that over the years, he's shifted away from providing endodontic procedures. "As my practice grew, I started cutting out the procedures that weren't profitable or enjoyable to me," he says. "I feel that endodontists can do a much better job and that they are better able to keep up with the latest trends in care. My patients seem to appreciate the referral once I educate them about the necessity and explain the benefits of a highly trained specialist." Although many patients value receiving as much of their care as possible from one trusted location, when practitioners are presented with treatment challenges that risk procedural errors and poor outcomes, consultation and referral are always valid options.
Tools and Recommendations for GPs
The standards of practice are constantly evolving based on new evidence and technology. Therefore, in order to provide the most appropriate care, it is the responsibility of all practitioners to be lifelong learners. There are ample opportunities for practitioners to learn endodontic care during their predoctoral education in dental school; however, focusing on the intricacies of endodontics can prove difficult given the multiple learning tracks required for graduation. "As a result of all of the requirements of dental school, when students graduate, they often find themselves less than prepared in some specific areas of their education, and endodontics tends to be one of those areas," explains Allen Ali Nasseh, DDS, MMSc, a clinical instructor of postdoctoral endodontics at the Harvard University School of Dental Medicine and private practitioner in Boston, Massachusetts. "And since the pandemic, we've come to see endodontics as an essential service, so now, GPs who want to provide that service need to compensate for any lack of formal predoctoral education with additional education after school."
According to the AAE, information technology has transformed the profession of dentistry and placed added emphasis on the evidence-based practice model. Contemporary methods of education emphasize problem-solving and critical thinking skills and stress the importance of professional interactions and the benefits of multidisciplinary and interdisciplinary care. Specialized continuing education courses, online resources, textbooks, hands-on training programs, mentorship opportunities, and other learning opportunities are valuable tools that GPs can use to enhance their knowledge and skills in endodontics. "There are many endodontic cases out there that a GP can handle confidently and achieve successful results," remarks Duplantis. "But as with anything else, it is important to place value in furthering your education. This is especially important when we want to expand our offerings within our practices." The AAE provides educational tools, videos, and publications that are available to GPs and endodontists alike to continue to build their knowledge. There are also several well-known endodontists who create content geared toward GPs. In that vein, Seibert is the creator and host of the Dental Digest podcast, which helps dentists stay on the cutting edge of developing technology, materials, and education.
Of course, not all educational experiences are equally valuable. "If you're planning on attending a corporate-sponsored course where there's minimal tuition, you're likely facing an opportunity to listen to a product pitch rather than to receive unbiased education," Nasseh cautions. "However, depending on the instructor, some of these courses can still be very helpful in learning bits and pieces. Independent students are responsible for parsing information from multiple sources and organizing the relevant knowledge rather than having a program director or school administrator organize it for them."
In preclinical endodontics, having students practice on extracted teeth is a common teaching method. It can also be a useful way for GPs to gain experience before moving on to treating patients. "Working on extracted teeth is the best way to hone your skills and identify the limits of your new techniques and materials," says Nasseh. "This practice can provide practitioners with a wealth of information regarding clinical skills, techniques, and root canal anatomy along with the comfort of knowing that any mistakes will not be costly to an actual patient."
Continuing education in endodontics that incorporates advances in technology, materials, and equipment further improves providers' abilities to deliver high-level care. For example, when indicated, the use of cone-beam computed tomography (CBCT) in endodontics can significantly enhance visualization of the canal spaces. "My skills and understanding have continuously progressed through training and experience," says Enrico E. DiVito, DDS, a clinical instructor at the Arizona School of Dentistry and Oral Health and private practitioner in Scottsdale, Arizona, "and related improvements in technology have supported this growth. Magnification helps me see better, 3D CBCT improves my case selection, and multisonic irrigation technology has dramatically improved my ability to handle complex anatomy in a single visit."
The development of modern technologies that improve clinicians' abilities to visualize complex anatomies has contributed to the provision of safer and more efficient root canal treatments that require shorter clinical visits and result in greater patient comfort.1 For example, technologies such as CBCT and other methods of 3D modeling have helped to improve diagnosis and treatment planning as well as enabled an approach that is referred to as guided endodontics. "But more importantly, such technologies can disclose hidden difficulties and challenges in teeth and provide clinicians with better pictures of cases before they attempt to perform root canal therapy," notes Nasseh.
Indeed, the use of innovative technology is fostering in a new era of endodontic care, enabling GPs and endodontists to perform treatments with increased sophistication and precision, which ultimately benefits patient outcomes. New irrigation systems, for example, are providing new levels of cleaning capabilities that positively impact both success rates and patient experiences. "The consistency and predictability have opened up opportunities for combined treatments that we did not have before," says DiVito. "Using multisonic irrigation and CAD/CAM technology, I can now perform a root canal, complete a buildup, and place a crown in one appointment and get a predictable result. Patients really appreciate the convenience and comfort of that level of care. We are doing these types of cases routinely now, and it has changed our scheduling and workflow. It's all been made possible by effectively utilizing the latest technology."
Because new materials and equipment can be expensive and/or have steep learning curves, GPs who wish to perform endodontic treatments should consider the amount of money and time that they are willing to invest to meet the standard of care. "The majority of endodontists are now treating with the aid of a microscope," explains Duplantis. "This is elevating the level of care and should now be seen as the standard of care. I was not willing to make that investment because I have a good referral network that can provide that level of care."
When GPs and endodontists form synergetic partnerships, it helps to ensure comprehensive patient management, and the GPs judiciously refer cases to specialists when indicated. "Communication is such an important piece of the puzzle," emphasizes Pryles. "Some of the best interactions that I have had during consultations are with patients whose GPs have clearly explained why they're meeting with a specialist."
DiVito concurs. "The best specialists recognize and respect GP efforts to provide quality care for their patients and will facilitate that through education, counseling, and treatment," he says. "Open communication is imperative."
Prioritizing Patient Well-being
In the dynamic field of dentistry, the boundaries between GPs and specialists, such as endodontists, are constantly evolving. Nonetheless, these boundaries should be respected. For GPs who provide endodontic treatment, determining the appropriate course of action for endodontic cases requires careful consideration of various factors, including case complexity, practitioner expertise, and available resources.
"We all need to know our strengths and weaknesses," concludes Duplantis. "As GPs, we should thoroughly assess each case and ask ourselves if we can treat it as well as an endodontist. If the answer is ‘no,' then it's best to refer." He cautions GPs to not attempt procedures without being 100% confident that the result will be a success. "The cost associated with failure is much greater than the profit from performing questionable procedures."
Moreover, the standard of care in endodontics is contextual in that it is shaped by the expertise available within given geographic areas and other factors. GPs must strive to uphold the standard of care and recognize when specialist intervention is necessary to ensure the best possible outcomes for their patients. Effective communication and collaboration between GPs and endodontists is essential to achieving this goal. By fostering open dialogue and mutual respect, practitioners can work together to provide comprehensive and seamless patient management.
The landscape of endodontic care is characterized by a delicate balance between competence and humility. All practitioners should continually educate themselves, leverage advancements in technology and materials, and above all, prioritize patient well-being. In doing so, they can navigate the complexities of endodontic care with confidence and integrity.
References
1. Decurcio DA, Bueno MR, Silva JA, et al. Digital planning on guided endodontics technology. Braz Dent J. 2021;32(5):23-33.