
Tissue Management Using Ultradent Products
Achieving profound hemostasis is critical in crown-and-bridge and operative dentistry.
Effective tissue management is one of the most important components of operative dentistry, including crown-and-bridge dentistry. Inadequate tissue management leads to poor impressions and poorly fitting margins. The natural result, the ill-fitting restoration, can jeopardize the surrounding soft tissue and the adjacent tooth structure, complete with the eventuality of recurrent decay.
Hemostasis
The first step in this process is achieving hemostasis. Ferric sulfate functions with a mechanism independent of normal clotting factors. This makes it also advantageous when controlling difficult surface capillary bleeding. Ferric sulfate solutions are best delivered in a syringe with a specially designed tip (eg, Metal Dento-Infusor tip, Ultradent Products, Inc.). This tip is not only used as an applicator, but also as a scrub brush. Pushing on the plunger and scrubbing with the tip moves the ferric-sulfate solution within the cut capillary orifice while simultaneously scraping off extraneous coagulum at the cut tissue. The result is “active” or profound hemostasis achieved by the formation of the individual microscopic coagulum plugs within each capillary and with all extraneous coagulum wiped clean from the surface.
Tissue Displacement
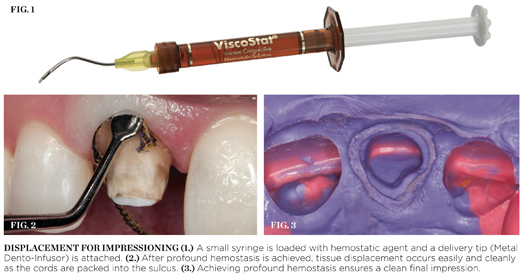
To begin tissue displacement, materials are prepared, including attachment of a delivery tip (Metal Dento-Infusor) to a small syringe and loading the syringe with a hemostatic agent (eg, Visco Stat, Ultradent Products, Inc.) (Figure 1). The clinician enters the bleeding sulcus with the syringe, circling the preparation: rubbing, scrubbing, and pressing firmly against the soft cut tissues while expressing material through the delivery tip. It is important to note that while it might seem counterintuitive to rub a bleeding area in order to achieve hemostasis, scrubbing with appropriate firmness is crucial to the success of this procedure. Rubbing firmly inside of the cut capillary opening will scrub away excess coagulum, allowing the hemostatic agent to reach the cut tissue. A simple and gentle painting motion will leave a lot of coagulum and the bleeding will not stop. If the cord is removed and the tissue bleeds, it means that the hemostatic was not rubbed firmly enough before the cord was packed. After circling the preparation for 30 to 60 seconds, new coagulum ceases to form, indicating that the bleeding has stopped and the capillaries are sealed. A firm air/water spray and suction are used to clean the preparation and to act as a test; if the preparation bleeds from a firm water spray, it will also bleed the moment it is touched with impression material or, in the case of operative dentistry, the moment the adhesive applicator touches the tissue. If bleeding is reinitiated in the test, the clinician should reapply the hemostatic agent and follow with another firm spray, never moving forward with the procedure until profound hemostasis had been achieved.
After the realization of profound hemostasis, tissue displacement occurs easily and cleanly as the cords are packed into the sulcus (Figure 2). Twisted or braided retraction cords handle differently from a knitted cord (eg, Ultrapak, Ultradent Products, Inc.). A knitted cord’s fibers run in more of a cross-sectional direction to the long axis due to the design of its interlocking loops. These loops have the ability to hold significant displacement and hemostatic fluid, while compressing nicely into the sulcus. The cord only remains in the sulcus for 1 or 2 minutes because displacement is the only goal; some of the rubbery nature of the collagen was already eliminated through obtaining hemostasis with the applicator tip, so the tissues were conditioned not to spring back once the cord was removed. After achieving retraction, the cord is removed and the preparation is sprayed firmly with air and water. The clinician ensures that profound hemostasis is still in existence; washes, dries, and makes the impression, always including a little bit of uncut tooth in the impression (Figure 3).
Control over fluids in the oral cavity—sulcular fluid, saliva or blood—is paramount to success in operative or crown-and-bridge dentistry. No contamination can be present in preparations through a bonding procedure. It is imperative that clinicians are in total control with tissue displaced appropriately for impression making. These guidelines help maximize the longevity of a restoration and are the responsibility of a quality professional; they help bring as much value as possible to the patients we serve, “treating our patients as we would like to be treated.”
Acknowledgment
Ultradent would like to thank Dr. Dan Fischer for authoring this article.
For more information, contact:
Ultradent Products, Inc.
Phone: 888-230-1420
Web: www.ultradent.com
Disclaimer
The preceding material was provided by the manufacturer. The statements and opinions contained therein are solely those of the manufacturer and not of the editors, publisher, or the Editorial Board of Inside Dentistry.



