

Treatment of the Class V Lesion: Crown Lengthening or Crown Shortening?
Timothy J. Hempton, DDS; Dimitrios Drakos, DDS; Philip J. Koralishn, DDS; Raymond Martin, DDS
Defects in tooth structure at the cervical portion of the clinical crown can occur as a result of caries, abrasion, chemical erosion, gingival recession, or abfraction. Class V caries occur on the buccal and lingual aspects and may extend subgingivally, limiting the therapist’s ability to remove them completely and place a proper restoration. Non-carious lesions, such as abfractions, may also extend subgingivally.
The exposure of dentin in the cervical portion of the tooth caused by caries, non-carious lesions, or periodontal attachment loss may result in root sensitivity and possible continued destruction of tooth structure. Dentin is less mineralized than enamel and, therefore, less resistant to acid degradation. Composite restorations are often utilized as a treatment for cervical caries or non-carious Class V lesions. This therapy is provided to reduce or eliminate sensitivity and prevent further destruction of tooth structure.
In circumstances where Class V lesions extend subgingivally, periodontal crown lengthening surgery may be employed. To predictably expose the lesion, repositioning the attachment apparatus via an apically-positioned flap, in combination with osseous resection, may be needed. In order to facilitate a more secure restoration, undercuts may be placed in sound tooth structure. Additional removal of tooth structure to facilitate restorative treatment and concomitant resection of supporting periodontal tissue can be described as subtractive therapy.
An alternative to placing restorative material for Class V lesions can be found in regenerative periodontal surgery, which is biologically reconstructive in nature. Predictable coronal positioning of the free gingival margin with concomitant attachment subsequent to caries removal can be achieved through surgical intervention.1,2 Commonly known as root coverage procedures, they are essentially crown-shortening procedures.
The purpose of this paper is to describe anatomical considerations that would direct a therapist toward utilization of a crown-lengthening procedure or a crown-shortening procedure to achieve health, function, and esthetics. Two contrasting cases are presented to illustrate the advantages and limitations of subtractive and reconstructive therapy.
Clinical Crown Lengthening: A Review
Surgical exposure of a Class V lesion can be achieved via a gingivectomy or an apically- positioned flap. Factors that influence the therapist’s decision in choosing one procedure over the other include the occlusal-apical height of gingiva and the location and thickness of the underlying osseous tissues. A minimum occlusal-apical height of 5 mm of gingiva, with 3 mm of attached gingiva adjacent to subgingival restorations, has been recommended.3 A biologic width of 3 mm is recommended between the most apical extent of a restorative margin and the osseous crest.4
Preservation of the existing band of keratinized tissue that is less than or equal to 5 mm, as well as access to the underlying osseous tissues, would require flap elevation for recontouring. A predictable crown-lengthening procedure occurs when positive osseous contours are established with the osseous crest located 3 mm from existing and proposed restorative margins.5,6
In the presence of periodontal health, the interdental osseous tissues would already be coronal to the interproximal osseous structures. Parabolic osseous contours on the facial and lingual aspects of the dentition, which are apical to the flat or convex contours in the interdental area, define positive architecture. In the case of the true Class V lesion occurring in periodontal health, interdental tissues do not need to be accessed if the caries, fracture, or abfraction does not encroach on the proximal surfaces of the tooth. The therapist need only recontour on the facial aspect a scalloped osseous crest, in an apical direction 3 mm from the proposed Class V restorative margin.
Clinical Case I: Crown Lengthening
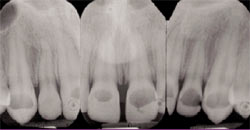
A 27-year-old male presented with Class V carious lesions located on the facial aspects of the maxillary anterior dentition and premolars (Figure 1). The patient did not report any medical conditions and was not a smoker. Clinical and radiographic evaluation did not reveal any attachment loss or bone loss. Subsequent to anesthetizing the patient, subgingival probing of the involved dentition with an explorer revealed a glassy hard surface consistent with enamel. A periodontal probe was utilized to sound to the cemento-enamel junction (CEJ), which was noted to be approximately 3 mm apical to the free gingival margin. Periapical radiographs indicated several millimeters of enamel, on average, located apical to the lesions and on the aproximal surface of the involved dentition (Figure 2).
These clinical and radiographic findings led to a diagnosis of incomplete passive eruption. Surgical excision of the appropriate amount of soft and osseous tissues can facilitate restorative therapy when subgingival caries is present. Therefore, flap elevation to allow for evaluation and possible alteration of osseous contours was treatment planned.
A scalloped incision was performed following the contours of the CEJs of the involved teeth that were sounded (Figure 3). As the patient had a 6-mm to 7-mm band of keratinized tissue, a margin of gingiva was removed to create flap contours that would match the contours of the CEJs. Following elevation of the facial flap, the anatomical crowns were fully exposed.
Two millimeters to 3 mm of enamel was present apical to the caries (Figure 4). It was noted that the osseous crest was within close proximity to the CEJ on multiple tooth sites. In order to facilitate a predictable outcome and prevent rebound of soft tissue coronally, the osseous crest was resected to an apical position, 3 mm from the CEJ. Because the patient did not have clinical attachment loss and radiographs indicated adequate bone height, the interdental tissues were left intact. Subsequent to ostectomy, positive osseous contours were established on the facial aspects of the treated dentition (Figure 5).
The flap was then positioned apically and sutured with 5-0 silk (Figure 6). At 3 months, the patient was referred to the general dentist for placement of composite restorations (Figure 7). A 3-month waiting period is recommended because no significant positional changes of the free gingival margin will occur after that period.7
Clinical Crown Shortening: A Review
Anatomy of root exposure
Coverage of exposed root surfaces was first described in the 1960s using the sliding pedicle flap.8 A classification system for predictable root coverage utilizing free gingival autologous grafts from the palate has been described that allowed for predictable root coverage irrespective of the width and depth of the root exposure, as long as the interdental tissues were intact (e.g., Miller Class I and II).9 The basic premise is that interdental tissues would provide an additional blood supply for nutrient support for the free graft.
Root coverage flap techniques
Prior to Miller’s work, a 2-stage procedure was proposed in which a free gingival graft was placed apical to the free gingival margin and subsequently coronally positioned.10 Advancement of the flap is achieved via a partial thickness flap which was dissected apical to the mucogingival junction. In the 1980s, others demonstrated that flaps positioned over connective tissue grafts could result in a predictable outcome for root coverage procedures in Miller Class I and II root exposures.11 Recently, another key to success was release of flap tension, as well as a minimum flap thickness of about 1 mm.12
Root surface modification
Decontamination of the root surface was initially achieved via root flattening with hand and rotary instrumentation, as well as use of citric acid.13 Ethylenediaminetetraacetic acid (EDTA) and tetracycline for root decontamination have also been investigated. However, studies comparing these 2 agents, as well as citric acid, to root planing have not demonstrated any clinical benefits.14 It was also demonstrated that excessive removal of root structure with scaling and root planing was no longer necessary, and that root decontamination of non-carious lesions could be achieved with polishing.15
Nature of the attachment
The nature of the attachment between the surface of the root previously exposed to the oral cavity and the grafted tissue has been described in many histological studies. It has been reported to be a fibrous adhesion,16 a long junctional epithelial attachment,17 or the combination of some regeneration, adhesion, and long junctional epithelium.18 Despite the nature of the attachment, it has been demonstrated that root coverage is successful over the long term and tended to improve with time (i.e., coronal creep of the healed graft).19
Roots with caries, abfractions or previous restoration
Three cases involving the removal of previously placed composite Class V restorations, followed by thorough root planing, have been described.20 Flaps were advanced over connective tissue grafts in order to achieve ideal tooth length. Furthermore, there is evidence showing that coverage of previously carious roots is as predictable a procedure as coverage of intact roots.21
Clincal Case II: Crown Shortening
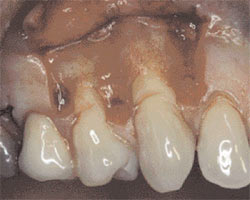
A 43-year-old, healthy, non-smoker male presented with non-carious Class V lesions on teeth #5 through #12 (Figure 8). The patient reported root sensitivity, as well as dissatisfaction with clinical tooth length. The involved dentition were treated in 3 separate procedures. This first procedure involved teeth #5 and #6. Vertical releasing incisions were placed mesial to tooth #4 and distal to tooth #7. The vertical releasing incisions extended apical to the mucogingival junction. A full-thickness flap was elevated to the level of the mucogingival junction. Apical to this level, a partial thickness dissection was performed to release tension on the flap and facilitate coronal positioning. There was notching of the roots, with significant loss of dentin in a V-shaped configuration (Figure 9). The root surfaces were smoothed with high-speed diamond rotary and hand instrumentation to achieve decontamination and facilitate flap adaptation. The enamel was recontoured with a finishing bur to create a more clinically acceptable CEJ (Figure 10).
A connective tissue graft was harvested from the right palate in the area of teeth #2 and #3. The graft was placed over the recontoured root surfaces and tacked into position bilaterally utilizing resorbable sutures (Figure 11). Subsequent to stabilization of the connective tissue, the tension free flap was advanced coronally to approximate the de-epithelialized papillae in the interproximal areas. The flap was sutured into position passively utilizing 5-0 silk sutures (Figure 12).
In a similar fashion, teeth #11 and #12 were also treated with connective tissue graft placement under a coronally advanced flap. The maxillary anterior dentition, including teeth #7, #8, #9, and #10, were simply treated with a coronally advanced flap. At 6 months, a photograph of the healed area was taken, demonstrating significant root coverage (Figures 13a and 13b). The patient was satisfied with the improved esthetics and elimination of root sensitivity.
Conclusion
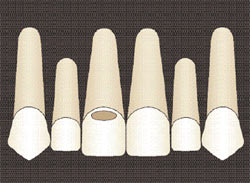
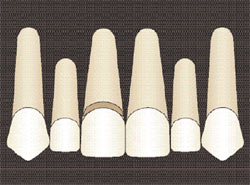
These 2 clinical cases represent contrasting management for the treatment of Class V lesions. Deciding which procedure to use depends upon the location of the CEJ. If the lesion is coronal to the CEJ (Figure 14) and located subgingivaly, the therapist can employ a crown lengthening procedure. By contrast, if the Class V lesion is located apically to the CEJ (Figure 15) and does not extend to the proximal surface of the tooth, gingival augmentation and concomitant clinical attachment can be utilized as a biologic alternative to placement of a composite restoration. The percentage of success for crown shortening, however, is contingent upon the anatomy of the interdental hard and soft tissues.
In between these 2 extremes, a therapist may find an obliterated CEJ due to the extension of caries from a point coronal to the CEJ to a point apical to the CEJ (Figure 16). In this case, the desired occlusal apical length of the clinical crown would be determined by the therapist. Esthetic factors, such as ideal tooth length for a given tooth and the relative location of the adjacent CEJs, should be considered. These parameters facilitate determination of the apical extent of the restorative material and coronal extent of the grafted tissue.
An additional factor to consider when choosing between a crown-shortening procedure or placement of a composite restoration on the root surface is the potential for degradation of resin-dentin bonds over time. Degradation of resin-dentin bond structures occurs after aging in the oral cavity.22 In non-esthetic areas, other materials such as amalgam could be considered if the apical extent of the lesion resides on dentin.
References
1. Camargo PM, Lagos RA, Lekovic V, et al. Soft tissue root coverage as treatment for cervical abrasion and caries. Gen Dent. 2001;49(3): 299-304.
2. Reiser GM, Bruno JF. The subepithelial connective tissue graft for achieving root coverage. In: Nevins M, Mellonig JT, eds; Periodontal Therapy, Clinical Approaches and Evidence of Success. Carol Stream: Quintessence Publishing Co., Inc.; 1998:355-364.
3. Maynard JG Jr, Wilson RD. Physiologic dimensions of the periodontium significant to the restorative dentist. J Periodontol. 1979;50(4):170-4.
4. Ingber JS, Rose LF, Coslet JG. The “biologic width”—a concept in periodontics and restorative dentistry. Alpha Omegan. 1977;70(3):62-5.
5. Palomo F, Kopczyk RA. Rationale and methods for crown lengthening. J Am Dent Assoc. 1978;96(2):257-60.
6. Rosenberg ES, Garber DA, Evian CI.Tooth lengthening procedures. Compend Contin Educ Dent. 1980;1(3):161-72.
7. Lanning SK, Waldrop TC, Gunsolley JC, et al. Surgical crown lengthening: evaluation of the biological width. J Periodontol. 2003;74(4):468-74.
8. Sugarman EF. A clinical and histological study of the attachment of grafted tissue to bone and teeth. J Periodontol. 1969;40(7):381-7.
9. Miller PD Jr. A classification of marginal tissue recession. Int J Periodontics Restorative Dent. 1985;5(2):8-13.
10. Bernimoulin JP, Lusher B, Muhlemann HR. Coronally repositioned periodontal flap. Clinical evaluation after one year. J Clin Periodontol. 1975;2(1):1-13.
11. Langer B, Langer L. Subepithelial connective tissue graft technique for root coverage. J Periodontol. 1985;56(12): 715-20.
12. Baldi C, Pini-Prato G, Pagliaro U, et al. Coronally advanced flap procedure for root coverage. Is flap thickness a relevant predictor to achieve root coverage? A 19-case series. J Periodontol. 1999;70(9): 1077-84.
13. Miller PD Jr. Root coverage using a free soft tissue autograft following citric acid application. Part 1: Technique. Int J Periodontics Restorative Dent. 1982;2(1):65-70.
14. Mariotti A. Efficacy of chemical root surface modifiers in the treatment of periodontal disease. A systematic review. Ann Periodontol. 2003;8(1): 205-26.
15. Pini-Prato G, Baldi C, Pagliaro U, et al. Coronally advanced flap procedure for root coverage. Treatment of root surface: root planing versus polishing. J Periodontol. 1999;70(9):1064-76.
16. Bruno JF, Bowers GM. Histology of a human biopsy section following the placement of a subepithelial connective tissue graft. Int J Periodontics Restorative Dent. 2000;20(3):225-31.
17. Majzoub Z, Landi L, Grusovin MG, et al. Histology of connective tissue graft. A case report. J Periodontol. 2001;72(11):1607-15.
18. Harris RJ. Successful root coverage: a human histologic evaluation of a case. Int J Periodontics Restorative Dent. 1999;19(5):439-47.
19. Harris RJ. A short-term and long-term comparison of root coverage with an acellular dermal matrix and a subepithelial graft. J Periodontol. 2004;75(5):734-43.
20. McGuire MK. Soft tissue augmentation on previously restored root surfaces. Int J Periodontics Restorative Dent. 1996;16(6):570-81.
21. Goldstein M, Nasatzky E, Goultschin J, et al. Coverage of previously carious roots is as predictable a procedure as coverage of intact roots. J Periodontol. 2002;73(12):1419-26.
22. Hashimoto M, Ohno H, Kaga M, et al. In vivo degradation of resin-dentin bonds in humans over 1 to 3 years. J Dent Res. 2000;79(6):1385-91.
 |
 |
|||
| Figure 1 Preoperative view of a 27-year-old patient with incomplete passive eruption and subgingival Class V lesions. | Figure 2 Radiographs of the maxillary anterior dentition indicate that caries do not extend apical to the CEJ. | |||
 |
 |
|||
| Figure 3 Internal bevel incision on the facial, from teeth #5 to #12. | Figure 4 View subsequent to flap elevation and prior to osseous resection. | |||
 |
 |
|||
| Figure 5 Osseous resection is performed to uncover the Class V lesions and establish a biologic width. | Figure 6 The mucogingival flap is sutured apically, exposing the anatomical crowns. | |||
 |
 |
|||
| Figure 7 After 3 months, the Class V lesions are restored with composite restorative material. Partial diastema closure has been achieved. | Figure 8 Preoperative view of a 43-yearold patient with generalized non-carious Class V lesions. | |||
 |
 |
|||
| Figure 9 A tension-free flap is elevated apical to the mucogingival junction, revealing the extent of notching in the roots. | Figure 10 Roots are planed and moderately recontoured. | |||
 |
 |
|||
| Figure 11 A connective tissue graft is tacked over the exposed root surfaces. | Figure 12 The flap is coronally advanced and sutured to the de-epithelialized papillae. | |||
 |
 |
|||
| Figure 13a Six-month post-treatment view of coronally advanced flap on facial of teeth #5 and #6. | Figure 13b Six months post-treatment of maxillary anterior dentition and first premolars, the free gingival margin most closely approximates the CEJ of the involved dentition. | |||
 |
 |
|||
| Figure 14 The Class V lesion is coronal to the CEJ, and the caries is subgingival. Treat with crown-lengthening procedure and placement of a composite restoration. | Figure 15 When the Class V lesion is apical to CEJ, provide a root coverage procedure for crown shortening. | |||
 |
||||
| Figure 16 The Class V lesion is coronal and apical to CEJ. Treat with a combination of a crown-lengthening procedure and a crownshortening procedure. | ||||
| About the Authors | ||||
|
||||
|
||||
|
||||
|
||||





