
Clinical Aspects of iBond Self Etch
Adhesion techniques in dentistry remain the most important aspect in governing long-term success or short-term failure of bonded restorations. Control of all the variables is difficult and demands attention to detail. The multiple steps in the process of bonding compounded with the challenges of environmental control of the oral cavity and consistency of technique can and do affect the quality of results. Research has driven manufacturers to develop products and techniques in this area that minimize steps and variables that can contribute to clinical unpredictability. The development and research efforts of Heraeus-Kulzer, LLC (South Bend, IN) has resulted in a new and improved seventh-generation bonding agent, iBOND® Self Etch. iBOND Self Etch combines high bond strength, improved marginal sealing, and elimination of postoperative sensitivity in a simple application method.
Dentists must understand what occurs when tissue is cut, as well as the effects on that tissue when medicaments are applied to it. It is equally important to know the chemistry and properties of these products. For bonding procedures, there is no product and no step more important than the bonding agent and its application. The quality of the product is governed by its inherent properties of bond strength, handling, and long-term predictability under continuous wear. This article evaluates these aspects for iBOND Self Etch.
Strength
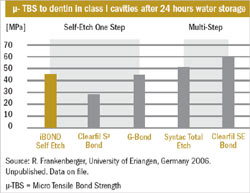
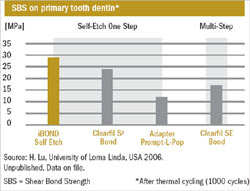
The consideration of bond strength is important with all cavity preparation designs for composite resins. A class I preparation has the advantage of four-wall support. However, class II, III, IV, and V preparation designs have less support and rely more heavily on materials (bonding agents) for retention. In any bonding endeavor, bond strength is the critical element. Without it, durability is questionable. iBOND Self Etch provides the highest bond strengths of the one-step formulations studied by Frankenberger1 (Figure 1). Further, Lu found high shear bonding strength to dentin2 (Figure 2), and Degrange found high initial shear bond strength to dentin3 (Figure 3). iBOND Self Etch can be applied to enamel and dentin; however, the enamel surface should be roughened or cut to attain the highest bond strength.
Handling
Clinical handling of iBOND Self Etch is simple and predictable. iBOND Self Etch is applied with only one coat. Its handling characteristics and formulation allow it to be spread evenly through air-drying, without the concern of it being puffed away. Its improved stability allows for room-temperature storage of an opened bottle, without demanding refrigeration.
Application of iBOND Self Etch is simple. First, the bottle must be shaken to incorporate all the components that may have settled between uses. Then, iBOND Self Etch is dispensed into a dry, clean well, dropping as much product as needed for the size and number of teeth to be restored. The bottle needs to be closed immediately after use to eliminate evaporation of the acetone in the formulation. A microbrush is dipped into the iBOND Self Etch and applied completely over the enamel and dentin. The layer is agitated to improve demineralization and diffusion of the bonding agent into the dentin and enamel of the prepared tooth. A light spray of clean, dry air is applied, leaving a glossy bright surface. The surface then is light-cured for 20 seconds.
INDICATIONS FOR USE
The indications for the use of iBOND Self Etch include:
- Bonding of direct composite restorations
- Bonding of indirect restorations in combination with light-curing luting cements
- Sealing of hypersensitive areas of teeth
Bonding of direct composite restorations is the most widely used application of iBOND Self Etch in most dental practices. Its ease of use and predictability of strength have made composite restoration techniques much more expeditious procedures than they were previously. Eliminating the steps of etching, rinsing, and applying bonding agent, along with the consideration of inconsistency each time these individual procedures are performed, has led to iBOND Self Etch’s widespread use for adhesion in restorative-based practices.
Bonding of indirect restorations in combination with light-curing cements is less frequently used, but also of great value. The chemistry of iBOND Self Etch necessitates the curing of the material with a light source. It cannot be used where light-curing is not a part of the procedure.
Sealing hypersensitive teeth has never been easier or more predictable. iBOND Self Etch is a successful material for sealing exposed root surfaces and, consequently, the elimination of adverse sensations in these areas. The iBOND Self Etch formulation contains monomers that can precipitate proteins, which close the dentinal tubules internally and thereby eliminate the pain pathway.
MARGIN INTEGRITY
Marginal discoloration is always a concern with composite restorations. With iBOND Self Etch, marginal discoloration is virtually eliminated because of the reduc- tion of water content in its formulation and the high content of monomers that evaporate more easily than solvents. Additionally, the consistency of iBOND Self Etch is improved because of its higher filler content, which results in a more homogenous adhesive layer. The resultant effects are higher bond strengths and improved marginal sealing. Because iBOND Self Etch contains acetone as its solvent, it provides an advantage over water-based bonding agents. Acetone is better able to carry the monomers deep into the tooth surface, thereby increasing the thickness of the hybrid layer and improving the bond.
CONCLUSION
Simplicity and predictability are a successful combination in the use of iBOND Self Etch for bonding procedures. Any time procedural steps can be eliminated and clinical results can be enhanced, the product’s design and formulation are winners. Its packaging and multiple uses make iBond Self Etch an integral part of the necessary armamentarium in esthetic restorative offices.
References
1. Frankenberger R. Unpublished data on file with Heraeus Kulzer, LLC. 2006.2. Lu H. Unpublished data on file with Heraeus Kulzer, LLC. 2006.
3. Degrange M. Unpublished data on file with Heraeus Kulzer, LLC. 2006.
For more information contact:
Heraeus Kulzer, LLC
Web: www.heraeus-kulzer-us.com
Phone: 800-431-1785
DISCLAIMER
The preceding material was provided by the manufacturer. The statements and opinions contained therein are solely those of the manufacturer and not of the editors, publisher, or the Editorial Board of Inside Dentistry. The preceding is not a warranty, endorsement, or approval for the aforementioned products or services or their effectiveness, quality, or safety on the part of Inside Dentistry or AEGIS Communications. The publisher disclaims responsibility for any injury to persons or property resulting from any ideas or products referred to in the preceding material.
 |  | |
| Figure 1 | Figure 2 | |
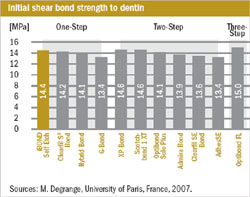 | Figure 1 through Figure 3 The results of several studies documenting iBond's high bond strengths to dentin. | |
| Figure 3 |

