
Xerostomia and the Critical Role of Saliva
Louis Malcmacher, DDS
Xerostomia, commonly referred to as dry mouth, affects nearly 10% of the United States population. This number reaches nearly 25% in patients 65 years or older.1 Defined as the subjective complaint of dry mouth,1 xerostomia interrupts regular functions of the salivary glands and can negatively impact the quality of life of those suffering from the condition. Although metabolic or immune disorders such as Sjögren’s syndrome can lead to xerostomia, the leading cause of dry mouth is medication use.2
This article will discuss the chemical make-up of saliva and its role in caries prevention and oral health, as well as how to collect a complete medical history in order to address potential causes of dry mouth when treating patients. It will also detail the additional concerns for cancer patients undergoing chemotherapy or radiation treatments. Finally, this article will address management options for the condition, and how dental professionals can help patients suffering from xerostomia improve their quality of life.
SALIVA
Saliva and xerostomia are closely linked, as dry mouth is typically associated with inadequate functioning of the parotid, sublingual, and submandibular salivary glands (Figure 1). Hyposalivation, the objective finding of a reduced salivary flow rate, irritates the mouth’s soft tissues, making them more susceptible to infection.3 It is important to note, however, that hyposalivation and xerostomia are not always related. Patients with hyposalivation may not report symptoms of dry mouth, and vice versa.
Not surprisingly, saliva is composed mostly of water. Making up 99% of saliva, water serves to moisten food so it can be swallowed easily and dissolves food molecules so that food can be tasted.4 The remaining 1% of saliva’s components include electrolytes (potassium and bicarbonate ions), mucus, enzymes (lysozyme), and anti-bacterial agents. Saliva’s non-water components play an important role in overall oral health, particularly caries prevention.4
- Electrolytes—such as calcium and phosphate ions—work to remineralize tooth enamel as well as help to modulate taste sensitivity and control pH.
- Mucus—acts as a lubricant to aid swallowing. Mucus also coats the mouth to prevent food from directly contacting epithelial cells in the mouth and esophagus.
- Enzymes—kill bacteria and prevent the overgrowth of oral microbial populations while aiding in digestion by breaking down starch.
- Antibacterial agents—act as a part of the immune defense system, including defensins that help prevent caries.
When salivary flow decreases, initial signs are often demonstrated by thrush (candidiasis), characterized by a white, cottage cheese-like plaque and reddened tongue.5 If left untreated, xerostomia can lead to burning sensations, rampant tooth decay, oral yeast infections, and halitosis.1
SALIVARY GLANDS
The salivary gland system is comprised of three glands: the parotid gland, sublingual gland, and submandibular gland. While saliva is produced in each, the different glands secrete a unique composition. As illustrated in Figure 1, the par-otid glands are located in each cheek in front of the ears, the sublingual glands beneath the tongue on the floor of the mouth, and the submandibular glands in the neck near the lower edge of each side of the mandible. Sac-like cell clusters called acini form the composition of each of the salivary glands, and signal the release of fluids.
This release of fluids is controlled by the parasympathetic and sympathetic nerves. Stimuli for increased salivation include the thought or smell of food, as well as food in the mouth. Conversely, a decrease in salivation can be caused by stress and anxiety.
COMPLETING A MEDICAL HISTORY
The prevalence of dry mouth increases as the number of prescription medications taken increases and with the number of medical conditions present. More than 400 medications have been proven to cause dry mouth.4 These include commonly prescribed medications for conditions such as high blood pressure and depression, as well as cancer treatments such as chemotherapy. The lowered salivary rate can lead to significant oral health issues, most notably an increased severity of root caries.6 Because patients are typically unaware that they are experiencing saliva reduction, they may not seek relief from their oral healthcare provider until complications such as caries, soreness, burning, or difficulty swallowing are present.1 As such, obtaining a detailed medical history for each patient is of utmost importance in the early diagnosis of xerostomia and/or hyposalivation.
Collecting a particularly detailed medical history becomes increasingly important with older patients who are typically taking a larger variety of medications for a number of ailments. This is especially true when assessing if a patient exhibits signs of dry mouth. A 2006 Dental Products Report survey found that 24% of the responding general practitioners noted xerostomia as the most common oral condition present in elderly patients.7 As such, taking a thorough medical history—which may include developing a medical history form specifically for elderly patients—can aid in the early identification of xerostomia symptoms, particularly when those patients are dealing with a complex variety of conditions.
CANCER TREATMENT AND DRY MOUTH
As previously mentioned, dry mouth is a common, significant adverse effect of cancer treatments such as chemotherapy. Patients undergoing cancer treatment may be increasingly subject to caries and other oral conditions. If a patient reports he or she is undergoing chemotherapy or radiation treatments, oral health professionals should thoroughly discuss treatment side effects and assess how to manage symptoms of xerostomia.
The severity of symptoms in a patient’s suffering from radiation-induced xerostomia is directly related to the radiation dose and dose rate. In many cases, the damage to the salivary gland is per-manent, even years after radiation therapy has terminated, and dry mouth symptoms become a life-long condition.8 As a result, it is important that patients are knowledgeable about a variety of management and treatment options for the condition.
DRY MOUTH MANAGEMENT AND TREATMENT
Research shows that patients suffering from dry mouth are most concerned with treatment options that provide long-lasting relief. Some mouthwashes and sprays, such as Oasis® Moisturizing Mouthwash and Oasis® Moisturizing Mouth Spray (GlaxoSmithKline Consumer Healthcare, Philadelphia, PA), have been proven to provide relief from the symptoms of dry mouth for up to 2 hours. Other over-the-counter (OTC) treatments include Biotène® Dry Mouth Mouthwash (Laclede, Dominguez, CA), and Salivart® Oral Moisturizer (Gebauer Company, Cleveland, OH). Additionally, travel-friendly treatments such as a mouth spray allow patients to manage their symptoms when treatments such as mouthwashes may be inconvenient or inaccessible. Further options include prescription treatments such as pilocarpine hydrocholide.
Although there is no proven cure for xerostomia, lifestyle changes and treatment options can ease the symptoms of dry mouth.
- Practice proper dental care.
- Sip water and other sugar-free liquids.
- Let ice melt in the mouth.
- Stimulate saliva flow with sugarless candy and/or chewing gum.
- Use a humidifier, particularly at night .
- Use a non-irritating mouthwash.
- Carry an oral lubricant.
- Discuss prescription treatments, such as pilocarpine and nicotinic acid tablets.
- Avoid caffeine.
- Refrain from using alcohol (including mouth rinses with alcohol) or tobacco.
- Eat soft foods and avoid spicy or acidic foods.
All of these treatment options may be used simultaneously to ensure optimal relief. While these treatments will not cure dry mouth, they may significantly improve the comfort and quality of life for dry-mouth sufferers.
CONCLUSION
Xerostomia is a prevalent condition; however, symptoms can be managed. Patients taking any type of medication—whether it is prescription or OTC—should be alerted to the symptoms and potential repercussions of dry mouth, most notably the increased risk of dental caries. Dentists also should complete a detailed medical history from all patients, particularly older patients, evaluating any symptoms of xerostomia and help to manage the condition before it worsens and/or impacts the patient’s overall oral health.
References
1. Guggenheim J, Moore PA. Xerostomia: etiology, recognition and treatment. J Am Dent Assoc. 2003;134(4):61-69.2. Atkinson JC, Baum BJ. Salivary enhancement: current status and future therapies. J Dent Educ. 2001;65(10):1096-1101.
3. American Dental Association. Oral health topics: Dry mouth. Available at: https://www.ada.org/public/topics/dry_mouth.asp. Accessed January 2, 2007.
4. Data on file. Research Triangle Park, NC: GlaxoSmithKline.
5. Hallenbeck JL. Pallative Care Perspectives. New York City: Oxford University Press; 2003.
6. Siegel MA, Silverman S, Sollecito TP. Clinican’s Guide to Treatment of Common Oral Conditions. 6th edition. Ontario, Canada: BC Decker; 2005.
7. Goff S. The new old. Dental Products Report. April 2006;42-48, 112-116.
8. Garg A, Malo M. Manifestations and treatment of xerostomia and associated oral effects secondary to head and neck radiation therapy. J Am Dent Assoc. 1997;128(8):1128-1133.
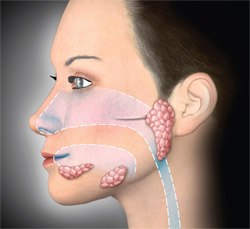 |
| Figure 1 Three major glands make up the salivary system: the parotid, sublingual, and submandibular glands. Along with these major glands, there are hundreds of minor glands beneath the lining of the lips, tongue, hard and soft palate, and inside the nose, cheeks, and sinuses that contribute to saliva production. |
| About the Author |
 Louis Malcmacher, DDS Louis Malcmacher, DDSPrivate Practice Bay Village, Ohio |

