
So What’s Next, 3-D Data Everywhere?
Anton Josef Voitik
This article is the first in a series of three.
More than a century ago, Ralph Waldo Emerson is reported to have said, “If a man can write a better book, preach a better sermon, or make a better mousetrap than his neighbor, though he builds his house in the woods, the world will make a beaten path to his door.”
The acquisition of medical three-dimensional (3-D) imaging data was revolutionized in 1973 with the invention of computerized tomography (CT) by Sir Godfrey Hounsfield.1 Initial CT scans took minutes per slice to acquire and hours for computers to generate images. Despite these limitations, the impact of CT on medicine was so profound that Dr. Hounsfield won the Nobel Prize in 1979, a mere 6 years after the publication of his first CT results.
In the 1980s, CT scans of the brain became the standard of care for brain imaging, replacing skull films and pneumoencephalography.2 This change was not without controversy in the literature of the early 1980s3 asking: Are skull films still necessary for a patient with head injury? CT won the debate and today skull films are extraordinarily rare. And it was only on an experimental basis that dental professionals and research-based product-oriented companies began to explore the use of scanned 3-D CT data at the time, with Calcitek, Inc. (Carlsbad, CA), serving as the best example where an early Stanford University software development was first used for computer-assisted design (CAD) and computer-assisted manufacturing (CAM) of lower jaw volumes, which the author used to manufacture subperiosteal implants for such well-known oral surgical specialists in implant dentistry as Golec, Hahn, and Babbush (Figure 1).4
The late-1980s saw the development of relatively rapid scanning, such that a single slice could be obtained in a breath-hold.5 This allowed scanning of the chest, abdomen, and pelvis to become a clinical reality. With this, a significant change in the workup modalities of many disease processes had become available.
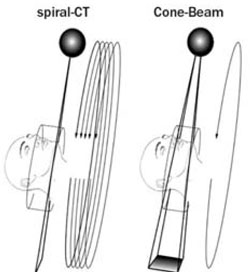
The early- to mid-1990s saw the development of spiral CT scanning and multi-slice CT scanning.6 With this new accelerated scanning ability, CT began to replace other older scanning methodologies, such as bone tomography.6 Scanner manufacturers also began to offer software applications specifically tailored for use in dentistry; that is, software that allowed the development of pre-set axial and oblique views usually specifically related to points on a panorama-like starting plane within an axial data set.
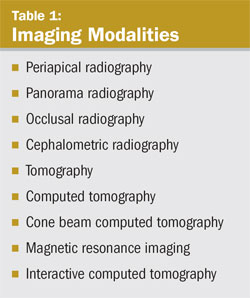
Some of the imaging modalities reported as useful in dentistry include:
- Periapical radiography, panorama radiography, occlusal radiography, cephalometric radiography, and tomography that make 2-dimensional (2-D) views of biologic systems possible;7,8
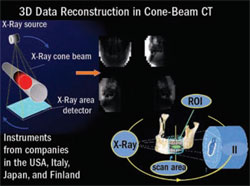
- Computed tomography, cone beam computed tomography, magnetic resonance imaging, and interactive computed tomography that make a 3-D look through a biologic system possible (Figure 2, Table 1).9
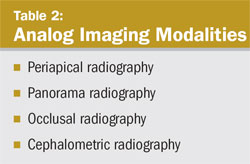
These modalities can be described as analog or digital and 2-D or 3-D. Most dentists are more familiar with analog 2-D imaging (Table 2).10
Analog imaging modalities are 2-D systems that rely on X-ray film or intensifying screens as the image receptors. Images can be produced digitally with the modalities listed in Table 1.
A 2-D image is best described as an image that has individual picture elements called pixels, and is described by its width and height in pixels (ie, 512 x 512).
Each pixel has a discrete digital value that describes picture intensity at that particular point. The value of a pixel element may be described as low as 8 bits (256 values) or as high as 12 bits (4,096 values) for black and white imaging systems whereas color imaging systems may go as high as 36 bits (65 billion values).
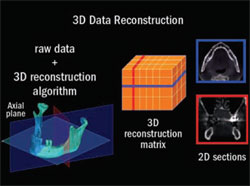
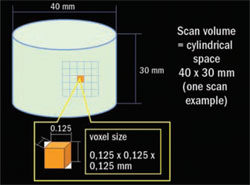
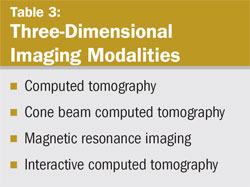
A digital 3-D image is described as an image matrix made up of individual image elements called voxels. Voxels are akin to Rubik’s cubes in that they not only describe the width and height (ie, 512 x 512) of imaged data but also represent its depth and thickness. An imaging volume or 3-D characterization of the patient is produced by contiguous images, which produce a 3-D structure of volume elements. Each volume element has an intensity value that defines its voxality potential. Typically, 3-D modalities have an intensity scale of 12 bits or 4,096 values. Table 3 lists the 3-D imaging modalities (Figure 3A, Figure 3B, Figure 3C).
In addition, for purposes of this article series, the following 3-D scanning modalities will be discussed.
- Advanced surface scanning that aims to make possible the previously academic in dentistry—a virtual impression;
- The use of rapid prototyping technology to reproduce volume avatars created in 3-D data sets with increasingly sophisticated mass-customization manufacturing processes.
The late 1990s and early 2000s have seen a continued increase in the diagnostic value of CT scanning, and CT scanning use is likely to continue to improve while per-scan costs decline.11 Already from 1998 to 2000, during the author’s dental-scan-data-use software development work at the Humboldt University’s Charité Hospital in Berlin, Germany, the use of CD-ROMs evolved as a very cost-effective carrier for dental patient data for the first time; data had to be made more easily accessible for transport between the scanning center and the steadily increasing number of early dental diagnostic software users. Up to this point in time, dental scanning data exchange and transport has relied on relatively costly and cumbersome media that had evolved for data transport among hospital scanning centers in the United States.
Given the increasing availability of 3-D data, dentistry and dental technology now have an opportunity for the first time to morph “surface dentistry and surface laboratory technology” into “systemic dentistry and laboratory technology” (Figure 4, Figure 5, Figure 6, Figure 7).
The use of reconstructed 3-D data also leads to a need for an understanding of the following:
- Cyberforming, a new utility for 3-D data.12
- Cybermolding, a support tool for mass customization.12
- Mass customization, a new manufacturing approach (Figure 8).12
CONCLUSION
In the future, especially if cone beam computerized tomography (CBCT) and interactive computed tomography (ICT) technology keeps replacing panoramic X-ray equipment technology at the near exponential rate it has shown since its introduction in the United States in 2000, it may come to pass that the numerous advantages of CBCT and ICT data handling firmly dictate a new standard of care for a multitude of clinical applications—dentistry included.
This is an important thought, as naysayers at every stop of this 3-D data utility evolution have been downplaying the value of CT, CBCT, and ICT with arguments regarding cost vs diagnostic benefit and the price of the technology. However, it has quickly become apparent to clinicians that 3-D data was and will increase to be immensely valuable, mainly because it increases diagnostic certainty. Dentistry is constantly plagued by risks involving uncertainty. The more confident the diagnosis, the more aggressive, streamlined, and confident the therapy.
REFERENCES
1. Autobiography of Godfrey Newbold Hounsfield (28 August 1919 ? 12 August 2004). Available at: https://www.nobel.se/medicine/laureates/1979/hounsfield-autobio.html. Accessed June 12, 2006.
2. Olson EM. CT revolution keeps on turning. RASLO Imaging Update. Radiology Associates of San Luis Obispo; May 2003.
3. Personal communications with Patrik Rogalla, MD, Head, CT Division, Department of Radiology, Humboldt University’s Charité Hospital, Berlin, Germany, 1997-2000.
4. Truitt HP, James RA, Lindley PE, et al: Morphologic replication of the mandible using computerized tomography for the fabrication of a subperiosteal implant. Oral Surg Oral Med Oral Pathol. 1988;65:499-504.
5. Sprals P Jr. Digital imaging systems and image processing. In: Physical Principles of Medical Imaging. Rockville, Md: Aspen; 1987.
6. Verstreken K, Van Cleynenbreugel J, Marchal G, et al. Computer assisted-planning of oral implant surgery; a three-dimensional approach. Int J Oral Maxillofac Implants. 1996;11:806-810.
7. Curry TS, Dowdy JE, Murry RC. In: Christensen’s Physics of Diagnostic Radiology. Philadelphia, Pa: Lea & Febiger; 1989.
8. Goaz PW, White SC. In: Oral Radiology: Principles and Interpretation, St. Louis, Mo: Mosby; 1992.
9. Swartz MS, Rothman SLG, Chafetz N, et al: Computed tomography in dental implant surgery. Dent Clin North Am. 1989;33: 555-597.
10. Kircos LT, Misch CE. Chapter on Diagnostic Imaging and Techniques. In: Dental Implant Prosthetics. St. Louis, Mo: Mosby; 2005.
11. Huang J, Bumann A, Mah J. Three-dimensional radiographic analysis in orthodontics. J Clin Orthod. 2005;39(7):421-428.
12. Voitik AJ. Prosthodontics in the Near and Distant Future— from 3D Data to Genetics. Opening Lecture to the General Session of the American College of Prosthodontists (ACP), Annual Meeting, Los Angeles, Ca; 2005.
 |  | ||||
| Figure 1 CAD/CAM of mandible and examples of possible superiosteal implant abutment solutions. | Figure 2 CBCT is an imaging option for diagnosis of complex maxillofacial anatomical situations at significant dose reduction levels without loss of image quality. | ||||
 |  | ||||
| Figure 3A Three-dimensional individual image elements are called voxels.Voxels not only describe the width and height (ie, 512 x 512) of imaged data but also represent its depth and thickness and are accessible to manipulation by advanced software envisioning tools. | Figure 3B Once acquired, voxel-based information provides fast, low-cost, and accurate data sets for “volume rendered” patient data reconstruction of avatars, of which certain aspects may be “segmented out” for diagnostic ease and visual clarity, as in the mandible shown. | ||||
 | 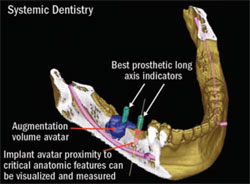 | ||||
| Figure 3C All currently available CBCT instruments allow precisely positioned regions of interest (ROI) and are an imaging option for diagnosis of complex maxillofacial anatomical situations at significant dose reduction levels without loss of image quality. | Figure 4 Bringing pertinent prosthetic tooth long-axis information into the scan via a scan template significantly improves its diagnostic value. | ||||
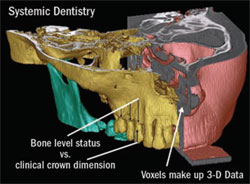 | 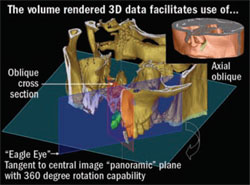 | ||||
| Figure 5 Three-dimensional data provides great patient education tools (eg, to demonstrate gingival pocket dimensions gathered from CT data in relationship to clinical crown length measurable on a patient’s study cast). | Figure 6 Volume rendered 3-D data facilitates the use of various planar views during a diagnostic conference now possible via interactive voice-over-internet-protocol among all treatment team members. | ||||
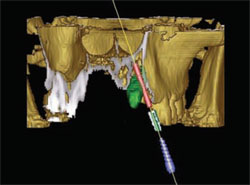 |  | ||||
| Figure 7 Volume rendered 3-D data facilitates clear diagnostic decision-making before surgery (eg, impacted cuspid will be removed to make placement of a dental implant in a planned, clinical treatment outcome-driven correct position). | Figure 8 Mass customization results from rapid prototyping application: 3-D printing. | ||||
 |   | ||||
| |||||


