

Using Resin-modified Glass-Ionomer Liners and Bases to Effectively Reduce Postoperative Sensitivity Under Direct Composite Restorations
Daniel H. Ward, DDS
Composite restorations have become the most popularly placed direct restoration in the United States.1 The public has increasingly demanded that esthetic restorations be placed and request them when a restoration is necessary. Unfortunately there has been a concomitant increase in reported postoperative sensitivity, which frustrates dentists and patients alike.
It has been reported that composite restorations exhibit greater technique sensitivity.2 Careful attention to detail is paramount but may be difficult in busy practices. Predictable, simplified techniques are needed, which would allow dentists to reliably place comfortable, long-lasting composite restorations.
VARIABILITY OF DENTIN BONDING
Great variability exists in the ability of resins to bond to dentin using the total-etch technique.3 Even when performed by knowledgeable clinicians, this method of dentin bonding can yield significantly varying results. At a conference several years ago (Key Educators Conference, Salt Lake City, Utah, March 1999), dental school faculty from throughout the United States were invited to use a number of different bonding agents to bond composite resin to extracted teeth under ideal laboratory conditions. The resulting restorations were loaded until debonding occurred using an Instron® machine (Instron Corporation, Norwood, MA). The forces applied were recorded. One popular dentin bonding agent provided strengths ranging from 7MPa to 46MPa (Figure 1). With such a divergence of results under ideal laboratory conditions performed by university-based teaching clinicians, how can predictable bonding results be expected in the active dental practice environment with many different treatment rooms and dental assistants?
One aspect often cited for the great variability in dentin bond strengths is the appropriate residual moisture of the dentin after the application and washing of the etchant. Collapsed collagen fibers are considered to contribute to the diminished bond strengths when the dentin is overdried.4 In addition, water droplets or “trees” are thought to inhibit optimal bond strengths when the dentin is left too wet.5 Different bonding systems advocate dissimilar methods for producing the optimal level of moisture on the dentinal surface before application of the bonding agents. Oftentimes, researchers in the laboratories of the manufacturers learn how to optimize the bond strengths of their particular products, but have a difficult time effectively communicating their methods to clinicians.
The proximity of the pulpal floor of the restoration to the pulp significantly affects bond strengths. The vast majority of the strength of the dentin bond is to intertubular dentin. At the dentin/enamel junction, the intertubular dentin is approximately 96% of the total surface area. In that area, there are approximately 2 million dentinal tubules/mm2 and the average diameter of the tubules is 0.4µm. As the proximity to the pulp is approached, the dentinal tubules become more abundant and larger in diameter. Near the junction of the dentin and the pulp, the intertubular dentin surface area is approximately 12%. At this point, there are approximately 4.5 million dentinal tubules/mm2 and the average diameter is 1.25 µm.6 This significantly different dentinal surface reduces the potential bond strength of resin to dentin and makes the complete sealing of opened dentinal tubules from acid-etching using the total-etch technique more challenging (Figures 2 and 3).
Overetching the dentin can create a deeper demineralized zone, which is more difficult to reseal with the application of the resin bonding solution.7 Most dentin bonding agents require a 20-second application of 37% phosphoric acid to the enamel, but only a 5-second application to the dentin. It is difficult to selectively apply the acid to different tooth structures. The dentin may be etched for a longer than ideal time when attempting to only etch enamel. Incomplete washing away of the etchant can leave acid within the dentinal tubules, an obvious source of irritation. Leaving the enamel thoroughly dry and the dentin moist, as recommended by many manufacturers, may also be a challenge. Restorations in deep areas are often located a great distance from the light, which cannot protrude into the deep areas. Inadequate polymerization of the light-cured resin can decrease dentin bond strengths as well as contribute to postoperative sensitivity.8
POSTOPERATIVE DENTINAL SENSITIVITY
It is believed that the primary cause of dentinal pain is fluid flow within the dentinal tubules.9 Opened tubules, which are then incompletely sealed during the operative and subsequent restorative phase of the treatment, allow fluid movement resulting in a painful stimulus. Multiple factors associated with the total-etch technique can contribute to postoperative sensitivity and no single simple solution exists to avoid it.
New generations of bonding agents have been developed in response to these concerns. Self-etching primers, used as part of the bonding process, have anecdotally been believed to reduce postoperative sensitivity.10 The reason cited for the decreased sensitivity is the dentinal tubules are never left open. As the etching solution penetrates through the dentinal tubules, the resulting debris from the demineralization of the dentin is incorporated with the depleted acidic monomer and seals the tubules. The reaction is self-limiting and only allows shallow penetration into the tubules (Figure 4). Self-etching techniques are effective at reducing sensitivity but the enamel margins are not as effectively etched because of a decreased concentration of acid.11 The resulting margins are susceptible to staining and premature degradation (Figure 5).
A technique is needed that can simply and reliably inhibit postoperative sensitivity yet offer superior marginal integrity over time. The sandwich technique has been advocated for many years but has been overlooked by many in search of the quickest and easiest methods.12 This technique involves placing a glass-ionomer liner or base in the deepest areas of the restoration and a composite material over this to complete the restoration. Although an additional step is involved, the possibility of longer lasting and more comfortable restorations may be worth the extra procedure.
USE OF RESIN-MODIFIED GLASS-IONOMER LINERS
Glass ionomers were introduced in the 1970s as an acid-base reaction cement. They set as a result of an acid-base chemical reaction and have been used as bases, liners, restorative materials, and cements. Advantages of glass-ionomer materials include fluoride release, bonding to dentin and enamel, and an expansion/ contraction rate similar to dentin.13 Early problems included postoperative sensitivity after crown cementation, slow setting times, low strength, and susceptibility to water contamination during the setting reaction phase. Modifications were made to improve some of these negative characteristics. Significant improvements to the working, handling, and strength characteristics were realized with the combination of the glass ionomer with a resin component. This new material was termed a resin-modified glass ionomer and included multiple polymerization modalities. Benefits included increased strength, reduced postoperative sensitivity, improved esthetics, and the ability to make the material dual-cured if desired. One disadvantage has been decreased fluoride release. A resin-modified, glass-ionomer material placed deep within a restoration and sealed with a composite restoration will have a limited ability to continually leech out fluoride ions. It has been reported that glass-ionomer–based materials can reuptake fluoride ions, an advantage for a cement or restoration exposed to the oral environment,14 but of limited consequence for sealed restorations.
A primary benefit of using glass-ionomer–containing materials is decreased postoperative sensitivity. When used without a priming agent, resin-modified glass ionomers do not open up the dentinal tubules (Figure 6). The bonding mechanism of a resin-modified glass ionomer to dentin is micromechanical and chemical.15 The bond strength of resin-modified, glass-ionomer material bonded to dentin compared with a resin material bonded to dentin in superficial dentin is significantly different. However, the closer the restorative interface to the pulp, the less the difference.2 Debonding and loss of restorations lined with a resin-modified glass ionomer covered by a composite outer layer has not been readily observed. Resin-modified glass ionomers do not have as significant polymerization shrinkage as dentin bonding agents or flowable composite materials, therefore, internal stresses are lessened. Reduced compressive strength exhibited by resin-modified, glass-ionomer materials is not critical when a restoration is covered with a composite restorative material. The function of the outer layer is to have high strength and excellent wear; the primary function of the deepest area of the restoration is to control postoperative sensitivity.
Great variability of dentinal surfaces exists. “Affected” dentin that is demineralized, but not bacteria-containing, is poor for conventional resin bonding.16 Resin-based dentin bonding should occur with ideal dentinal surfaces. Resin-modified materials allow a higher likelihood for successful bonding when the dentist is not sure that 100% of the altered dentin has been removed. When defective composite restorations have been removed, it has been the author’s observation that significant differences exist in the restorative/ dentinal interface between resin-bonded surfaces and glass-ionomer surfaces. Restorations containing glass ionomer exhibit less recurrent decay.
CLINICAL TECHNIQUE
In restorations where the restoration is deeper in several areas than ideal depth, a resin-modified, glass-ionomer liner may be placed (Figure 7). A resin-modified glass ionomer is mixed and placed to cover all of the deepest dentin (Figure 8) (3M™ Vitrebond™, 3M ESPE, St. Paul, MN). The material is thoroughly light- cured. The tooth is acid-etched, washed, and dried, and a bonding agent is placed. Then the definitive composite material is placed, cured, and finished.
In deeper and more extensive restorations, the use of a resin-modified base is extremely beneficial (Figure 9). The initial preparation is made to allow access to the carious area and to remove the faulty restoration. The use of a small round bur in a slow-speed handpiece is an excellent way to ensure that all of the decay has been removed (Figure 10). Once all the decay has been removed, an encapsulated machine-mixed material can be easily titrated and placed (GC Fuji II LC, GC America, Inc, Alsip, IL). The material should be quickly placed and thoroughly light-cured (Figure 11). The dual curing capability of the material ensures adequate polymerization even in the deepest areas. A high-speed handpiece is then used to remove any excess material on the enamel and the enamel margins are prepared to expose fresh enamel rods (Figure 12). The enamel part of the preparation is acid-etched for 20 seconds, washed, and dried thoroughly (Figure 13). The bonding agent is applied for 20 seconds (GLUMA® Comfort Bond + Desensitizer, Heraeus Kulzer, Inc, Armonk, NY), the solvent is evaporated, and light-cured for 20 seconds. The composite material is first warmed in a composite heater (Calset™, AdDent, Danbury, CT) to improve handling and polymerization conversion rates and then incrementally placed and cured (Figure 14) (AELITE™ Aesthetic Enamel, Bisco, Inc, Schaumburg, IL). The final restoration is finished, polished, and a surface sealant is placed (Figure 15). It has been the author’s experience that patients treated with large restorations have exhibited significantly less postoperative sensitivity with this technique.
CONCLUSION
The resin-modified, glass-ionomer liner and base should be considered an important part of a dentist’s armamentarium. Its ease of use, reduced technique sensitivity, and significant reduction in postoperative sensitivity warrant increased use. Instead of using new generations of bonding agents, which may compromise marginal integrity, we should revisit a simple solution that has been available for years.
REFERENCES
1. Berthold M. Restoratives: trend data shows shift in use of materials. ADA Newsletter. 2002;33(11):1.
2. O’Keefe KL, Pinzon LM. Management of the prepared tooth for placement of direct posterior composite restorations. Dent Today. 2005;24(9): 70-77.
3. Powers JM, O’Keefe KL, Pinzon LM. Factors affecting in vitro bond strength of bonding agents to human dentin. Odontology. 2003;91(1):1-6.
4. Gwinnett AJ. Dentin bond strength after air drying and rewetting. Am J Dent. 1994; 7(3): 144-148.
5. Tay FR, Gwinnett AJ, Wei SH. The overwet phenomenon: a scanning electron microscopic study of surface moisture in the acid-conditioned, resin-dentin interface. Am J Dent. 1996;9(3):109-114.
6. Gaberoglio R, Brannstrom M. Scanning electron microscopic investigation of human dentinal tubules. Arch Oral Biol. 1976; 21(6): 355-362.
7. Miller MB. Solving posterior composite sensitivity. Prac Periodontics Aesthet Dent. 1995;7(7):30.
8. Caughman WF, Rueggeburg FA, Curtis JW Jr. Clinical guidelines for photocuring restorative resins. J Am Dent Assoc. 1995;126(9): 1280-1286.
9. Brannstrom M. Sensitivity of dentine. Oral Surg Oral Med Oral Pathol. 1966;21(4): 517-526.
10. Denehy G, Cob D, Bouschlicher M, et al. Two-year clinical evaluation of a self-etching primer/adhesive in posteror composite. J Dent Res. 2002;81:A-80. Abstract 434.
11. Miguez PA, Castro PS, Nunes MF, et al. Effect of acid-etching on the enamel bond of two self-etching systems. J Adhes Dent. 2003;5(2): 107-112.
12. Davidson CL. Glass-ionomer bases under posterior composites. J Esthet Dent. 1994; 6(5):223-224.
13. Albers HA. Tooth Colored Restoratives. 9th ed. Hamilton, Canada: BC Decker, Inc; 2002:51.
14. Forsten L. Short and long-term fluoride release from glass ionomers and other fluoride-containing filling materials in vitro. Scan J Dent Res. 1990;98(2):179-185.
15. Yoshida Y, Van Meerbeek B, Nakayama Y, et al. Evidence of chemical bonding at biomaterial-hard tissue interfaces. J Dent Res. 2000;79(2): 709-714.
16. Nakajima M, Sano H, Burrow MF, et al. Tensile bond strength and SEM evaluation of caries-affected dentin using dentin adhesives. J Dent Res. 1995;74(10):1679-1688.
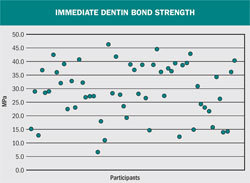 | |||||
| Figure 1 Variability of dentin bond strengths placed by different dentists. | |||||
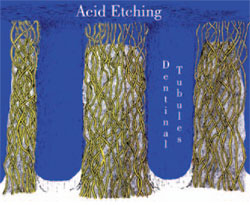 | 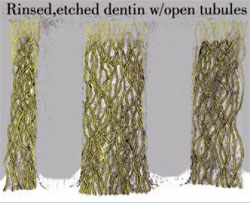 | ||||
| Figure 2 Acid-etching the dentin. | Figure 3 The opened tubules after etching the dentin. | ||||
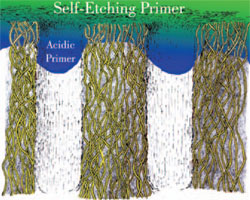 |  | ||||
| Figure 4 Self-etching primers etching and bonding. | Figure 5 The margins of a tooth restored using a self-etching primer. | ||||
 |  | ||||
| Figure 6 Unopened dentinal tubules covered with a glass-ionomer liner. | Figure 7 Fully excavated preparations. | ||||
 |  | ||||
| Figure 8 Preparations after a resin-modified glass ionomer was placed. | Figure 9 A faulty restoration. | ||||
 |  | ||||
| Figure 10 The use of a slow-speed round bur to ensure complete decay removal. | Figure 11 Bulk placement of a resin-modified, glass-ionomer base. | ||||
 |  | ||||
| Figure 12 The reprepared tooth after trimming of excess resin-modified, glass-ionomer base. | Figure 13 Acid-etching enamel. | ||||
 |  | ||||
| Figure 14 Final addition of the composite. | Figure 15 Completed, polished, and sealed restoration. | ||||
| |||||


