The Basics Still Matter
Fundamentals of removable prosthetics remain critical in digital workflows
Jennifer Vishnevsky and Jason Mazda
One of the hallmarks of digital dentistry is the way that increasingly intuitive software can make so many workflows easier and more efficient. With great power comes great responsibility, however, and as digital technology gradually replaces the conventional equipment, materials, and workflow processes utilized for removable prosthetics,1 the fundamentals of denture design and fabrication remain as important as ever. "Digital is our future," says veteran technician and educator Vincent Verderosa, MDT, CDT. "The problem is that anyone can learn to use the software, when in fact they also need to know the fundamentals of denture construction. The software can place teeth exactly where you mark a retromolar pad or cuspid area, which works for a Class I occlusion. For a Class II or Class III occlusion, however, you need to know the fundamentals of where the teeth belong—the crest of the ridge on the mandibular arch, two-thirds of the height of the pad, and all of the other principles we have learned over so many years."
Using digital technology as a crutch may seem tempting, especially for dentists and dental technicians who have previously focused more on crown-and-bridge but want to venture into new territory—and new revenue streams. "Dentists still need to have a clinical understanding because digital dentures are not the end-all-be-all to problem solving," says Kimberley Daxon, DDS, a Senior Faculty Member of The Dawson Academy.
While the required steps can be accomplished more efficiently with digital dentures than with conventional dentures—in as few as two visits instead of five—those steps cannot be skipped.
"What we are able to do now is not eliminate key steps, but combine them and become more efficient," says Brian Goodacre, DDS, MSD, Associate Professor at Loma Linda University School of Dentistry. "The dentist can combine a diagnostic impression and fabrication of a custom tray in one appointment, chairside with the patient, which provides advantages to the clinician and patient when done correctly."
A Focus on Fundamentals
Upholding the fundamentals begins with the clinical portion of the denture process.
"A conventional analysis is still necessary when evaluating the patient," Goodacre says. "Some people assume that because the workflow is digital, it can make up for bad records or missed information, but it does not. We need to make sure that we do not forget the principles on which dentistry was built."
According to McLaren and Culp, "Despite the modern age of digital smile design, [laboratories] still rely on sound concepts and principles of facial and dentofacial esthetics."2 Clinicians must focus on each aspect of dentofacial analysis, such as how to look at the face and smile, where the teeth are positioned within the face, incisal edge position, lip mobility, lip display, and lip length.
"Capturing borders and landmarks when making final impressions, as well as knowing where to position the teeth in the face and occlusal schemes, are critical concepts to the success of a removable restoration and carry through whether analog or digital techniques are being utilized," says Dean E. Kois, DMD, MSD, an Instructor at the Kois Center and a prosthodontist with a private practice limited to restorative, esthetic, and implant dentistry in Seattle, Washington.
The vertical dimension of occlusion (VDO) and centric relation record should be determined first.
"After that, the fundamentals of selecting a functional and esthetic tooth position and ensuring the denture has proper border extensions are concepts that do not change with digital technology," Goodacre says.
If an existing denture is being used as the basis for the new prosthetic, the VDO often needs to be re-established.
"Most dentists check a patient's VDO by marking the nose and the chin and measuring as the patient is biting down or the lips are just touching," Verderosa says. "They put the wax rims in and perhaps determine that they want to open the VDO by a couple millimeters. With a digital workflow, checking and often adjusting the VDO is still necessary."
Focusing on the correct landmarks is an effective way to ensure a well-supported denture. While dentists have some more leeway in regard to using a lingualized or flat plane for proper occlusion, their decisions must be based on a foundational knowledge. As with other aspects of the profession, it's up to a provider to focus on clinical decision making and reasoning in order to help a patient develop proper function.
"Regardless of how dentures are made, the clinician must have an understanding of whether the teeth are in the right position," Daxon says. "If a patient presents with a lisp, for example, then the dentist must know how to problem solve that."
Streamlining Data Acquisition
Digital processes introduce a number of efficiencies, including improved ability to work collaboratively with the entire dental team.
"We can now discuss acquired clinical and technical data in real time," says Robert Kreyer, CDT, Director of Advanced Dentures and Implants for MicroDental Laboratories. "Dentists open their email for online access to a proposed digital denture case plan previewer and then analyze the design in different virtual perspectives, while discussing prosthetic variables with the digital denture technician."
Many elements of the traditional workflow can be consolidated, but not eliminated. In the digital workflow, several steps can be condensed into fewer visits because all records can be taken during the first visit. In addition to the time savings—and subsequent cost savings—consolidating the steps also often reduces the chances for mistakes.3
"We have proven that we can cut steps," says Alexander Bendayan, DDS, Associate Dean and Clinical Professor at Boston University's Henry M. Goldman School of Dental Medicine. "That benefits both the dentist and the patient. Digital dentistry allows us to communicate with the laboratory faster. Overall, we are minimizing the number of appointments and maximizing the delivery of care."
It's important to note that even when these steps are combined, they cannot be skipped. "Most all of our digital techniques are adopted from our analog techniques," Kois says. "Digital dentistry is making us more efficient by consolidating office visits and moving information out of our offices through the internet rather than mail, but it is not substituting for our knowledge of dentistry. Moving to a digital workflow will not make you immune to errors."
Scanning the Edentulous Arch
As much as digital technologies can streamline processes, they can also pose new challenges, and the most significant one for dentures might be scanning the edentulous arch—to the point that a debate persists about whether or not it is even viable. Many digital denture workflows still utilize conventional impressions, with the laboratory digitizing the data via a desktop scanner. For those scanning intraorally, obtaining a quality scan is critical because poor impressions will lead to a poor-fitting denture.
"Dentists still need to understand anatomy when making preliminary impressions," Daxon says. "Knowing how to take a good border molded final impression is fundamental. That cannot be skipped. Soft-tissue supporting landmarks must be captured."
Verderosa says younger dentists who are embracing intraoral scanning must understand the level of function that is involved in a full denture.
"Getting the correct data is very important," Verderosa says.
Laboratories often manage with flawed impressions in analog workflows, but that becomes more difficult with digital scans.
"If we have a drag on a tooth in a conventional impression, we scrape the model, remove it, and proceed," says Tom Wiand, CDT, Owner of Wiand Dental Lab in Scottsdale, Arizona. "If you have a hole in a scan, that data does not exist, so the software cannot use A and C to figure out what B is. Dentists need to be more diligent than ever about really critiquing their impressions before sending them to the laboratory."
Although intraoral scanning of an arch with no teeth is challenging, Goodacre says it is viable.
"You will find that the maxilla is easier to capture than the mandible," he says. This is due to the increased attached tissue in the maxilla. In the mandible, you have the tongue and cheeks, which are constantly moving. The scanner cannot capture moving tissue, and you can struggle to capture the entire mandibular denture extension."
If a computer is not capturing movement or enough overextended tissue, Bendayan encourages marking in the patient's mouth.
"We can create a visual landmark for the digital workflow," Bendayan says. "That is a way to bypass something that the computer is not doing. There is a big market push to get to the point where the digital workflow can figure that out."
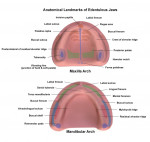
For technicians, understanding basic soft tissue anatomy is the foundation for success with complete dentures; if the necessary anatomy or biology of the denture space cannot be read easily in the negative impression, then it must be taken again until it is correct and all necessary soft tissue anatomy is visible.4 Anatomical landmarks such as the retromolar pads, external oblique, mentalis muscle, frenum attachments, mylohyoid ridge, tuberosities, hamular notches, incisive papilla, labial sulcus, and buccal vestibule are critical and must be captured in the positive (and easily read in the negative) aspect of any edentulous impression.4
"With conventional border molding, we ask patients to perform functional movements to determine the proper extension," Goodacre says. "When you are scanning, you need to approximate the denture border and hold the tissue in the desired extension while you scan in one pass. This emphasizes the need for proper patient selection, and while this may seem impossible, with practice it becomes easier."
Design and Fabrication
Experience is critical for laboratories as well. Some have speculated about the feasibility of teaching denture fundamentals to computer-savvy prospects from outside the dental profession, such as graphic designers, but Wiand says it has become clear that that is not the best option. A 30-year veteran technician himself, Wiand implemented an in-house milled denture system in his laboratory earlier this year.
"As the software becomes more intuitive, and there are more workflows than workarounds, training experienced technicians to design dentures digitally becomes easier," Wiand says.
Conversely, training someone from outside the dental profession on setting denture teeth is a tougher task.
"The software helps design teeth, but judgment calls are still necessary many times," Wiand says. "If you are making a full maxillary denture against natural mandibular dentition, is the arch form proportionate? Do the cusps of teeth Nos. 6 and 11 end in the proper position, along the long axis of the first bicuspids on the mandibular? Are they too wide, narrow, short, or tall? You might need to immediately adjust the mold to obtain an appropriate arch form. Then, the occlusal plane, which was set using landmarks, might be higher on one side than on the other. There is no way for a computer to propose perfect occlusion every time. You need to use the tools in the software to set teeth, just as you would with your hands traditionally: adjusting the camper's plane and the horizontal plane, positioning it buccolingually, and then individually extruding or intruding each tooth to achieve proper occlusion with the opposing arch. The same rules and average values apply as with traditional methods."
Verderosa notes esthetic details that experienced denture technicians have learned over the years. Tools exist in the software to apply this knowledge to digital designs, but it starts in the technician's head.
"Some patients might require a more feminine or masculine smile," Verderosa says. "Characterization and eminence are important. For example, I typically twist the laterals slightly for female patients because they often want a softer smile, while male patients tend to prefer bolder smiles with straight centrals for light to hit. Or, if you are savvy enough to recognize a cuspid eminence with little eminences around all the teeth, then you can scoop out in the flange area on the maxillary anterior, but you also want it a little full in the posterior so when the patient chews, the food comes off the side of the denture and back onto the occlusal table for chewing."
Class II and Class III cases require even more functional expertise, as well.
"The mandibular posterior teeth need to be on the crest of the ridge," Verderosa says. "Everyone prefers Class I in the maxillary posteriors, but if the teeth are going off the ridge and the occlusal pressure is not supported by bone, then the denture could fracture. Often, a cross-bite treatment is required. It's all about the fundamentals of denture construction, whether you are working with complete removable dentures, hybrid implant cases, or removable partials."
Beyond their own responsibilities, laboratories still need to be prepared for less-than-ideal clinical information from the dentist.
"If a dentist did not give you what you need every time in the analog world, they still will not in the digital world," Wiand says. "It is great if the dentist provides a wax rim that is contoured, but that is idealistic. There are many times when you need to rely on average values, such as the 22-mm distance from the vestibule to the incisal edge and the 5- to 7-mm distance from the incisal papilla to the facial. Experienced denture technicians have mastered that process."
Of course, the number of experienced denture technicians is dwindling. However, Wiand says digital technology makes it easier for young technicians to branch out into dentures.
"One thing these workflows accomplish is they decrease the necessity for manual dexterity," Wiand says. "Transferring information from your brain through your hands to a wax setup requires skilled hands. A trainee once told me setting teeth felt like stacking peas on top of each other. Balancing, securing, and manipulating teeth is difficult by hand, but not when you are using a mouse to grab a tooth and move it."
The Future Is Digital
Despite everything that needs to carry over from analog to digital denture processes, some elements can be left behind. Post dams, for example, may not be necessary in many cases.
"If the dentist utilizes proper border molding and compresses the soft tissue, then you should not need a post damn because digital dentures have negligible shrinkage," Verderosa says.
The flexibility and efficiency that software innovations, advanced manufacturing equipment, and next-generation materials bring to dentures will likely lead to CAD/CAM becoming as prevalent as it is for crown-and-bridge applications.5 With the benefits outweighing the negatives, increasing numbers of dental professionals are accepting that this workflow will continue to advance as long as fundamentals of prosthetics are maintained. The clinical performance of digital dentures in early studies has been promising with positive results in terms of both patient satisfaction and cost-effectiveness.6
Additionally, the digital workflow has improved the collaborative environment between dentists and laboratories, which is always crucial.
"The speed with which I can provide a set of impressions digitally and communicate with my laboratory is impressive," Bendayan says.
References
1. Kreyer R. Digital transformation of denture workflows. Inside Dental Technology. 2018;9(10):24-31.
2. McLaren E, Culp L. Smile analysis: the Photoshop® smile design technique: part I. J Cosmetic Dent. 2013;29(1):94-108.
3. Furuyama J. Digital dentures: efficient, well-fitting solutions for edentulous patients—a case report. Compend Contin Educ Dent. 2016;37(11).
4. Kreyer R. Edentulous soft tissue anatomy. Inside Dental Technology. 2018;9(2):42-48.
5. Fisker R. (2018). Making digitally designed and fabricated dentures a reality. Inside Dental Technology. 2018;9(1):50-51.
6. Anadioti E, Musharbash L, Blatz M, et al. 3D printed complete removable dental prostheses: a narrative review. BMC Oral Health. 2020;20(1):343.